Safety steps
Confirm AF, check for urgent symptoms, assess stroke risk, review bleeding risks and look for reversible triggers.
Treatment choices
AF treatment is not one thing. It can mean blood thinners to prevent stroke, rate-control medicines to slow the pulse, cardioversion to restore rhythm, rhythm medicines, catheter ablation, sleep-apnoea and blood-pressure work, alcohol reduction, weight management, and regular reassessment.
Key points
Confirm AF, check for urgent symptoms, assess stroke risk, review bleeding risks and look for reversible triggers.
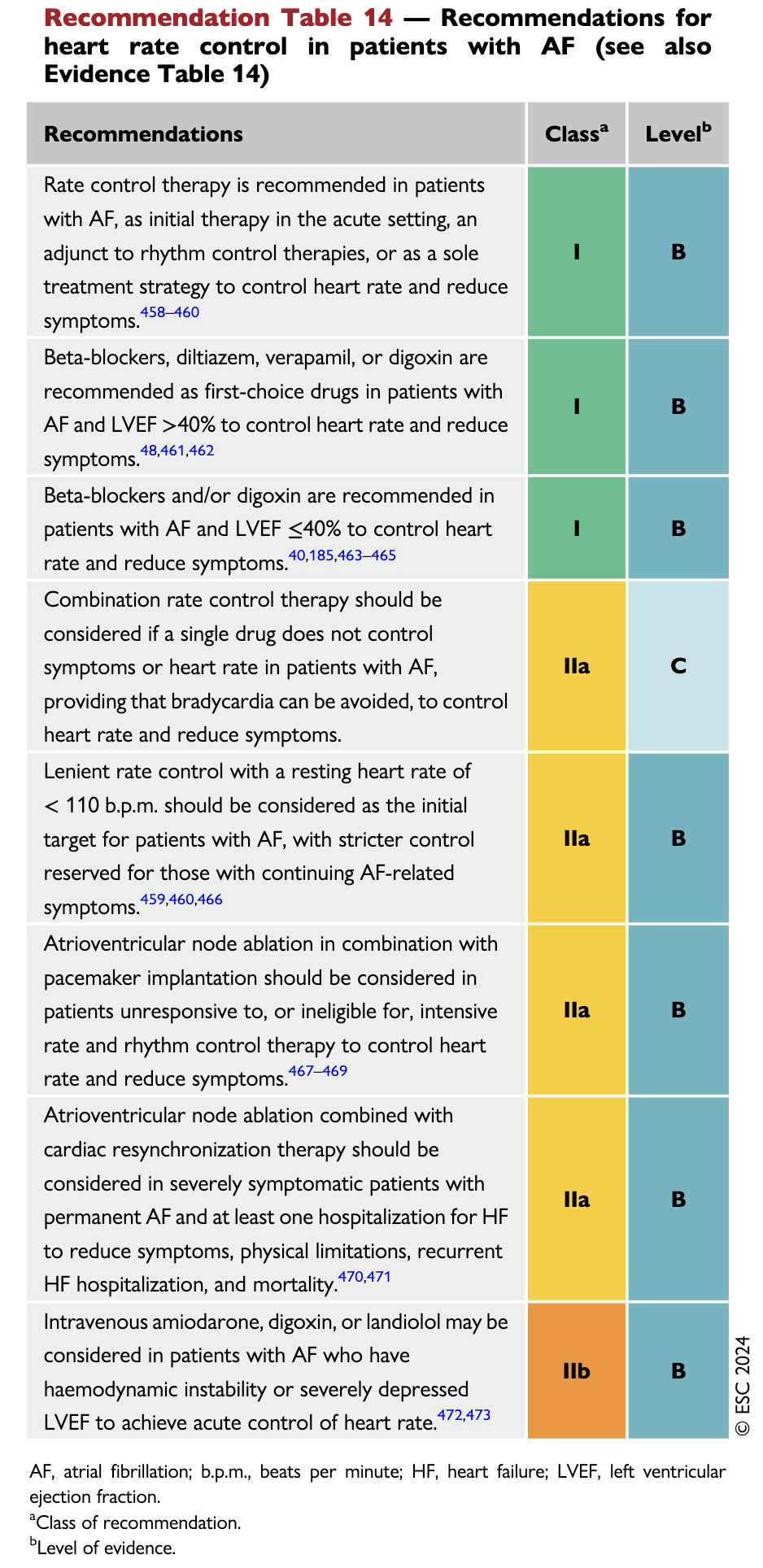
Medicines may slow the heart so symptoms, breathlessness or heart-failure strain improve even if AF continues.
Cardioversion, rhythm drugs and ablation try to restore or maintain sinus rhythm when symptoms, timing or heart function justify it.
Blood pressure, sleep apnoea, weight, alcohol, diabetes, thyroid disease and fitness can change recurrence risk.
For one patient the urgent issue is stroke prevention. For another it is a fast heart rate, heart failure, severe symptoms, recurrent AF after cardioversion or a strong preference to attempt sinus rhythm. Good AF care separates those problems instead of pretending there is one universal treatment ladder.
A planned electrical cardioversion may quickly show whether sinus rhythm improves fatigue, breathlessness or exercise tolerance. It may not last, but even a temporary response can help guide whether rhythm-control treatment is worth pursuing.
Modern guidelines increasingly support earlier discussion of catheter ablation in selected symptomatic patients, especially paroxysmal AF, but it is still a procedure with tradeoffs. The best decision depends on AF type, atrial size, heart disease, access, operator experience and patient goals.
Sleep apnoea treatment, alcohol reduction, blood-pressure control, weight management and fitness do not replace anticoagulation or cardiology review, but they can reduce AF burden and make cardioversion or ablation more durable.
Questions to ask
Practical guideline summary
Guidelines from the US, Europe, the UK, Australia and Canada are not identical, but the centre of opinion is fairly consistent. Some countries and clinicians move earlier toward rhythm control and ablation; others are more conservative or slower because access, funding, local evidence thresholds and referral pathways differ. This summary is a discussion aid, not a personal order set.
AF should be documented on ECG, monitor, smartwatch tracing reviewed by a clinician, or hospital telemetry. Do not build a whole plan on a vague palpitation description alone.
Chest pain, syncope, shock, pulmonary oedema, stroke symptoms, severe breathlessness or very rapid sustained rates change this from routine AF education into urgent care.
Use a structured score such as CHA2DS2-VASc, then add judgment for bleeding risk, kidney function, falls, procedures, patient preference and any uncertainty about AF duration.
Rate control is reasonable for many. Rhythm control is worth active discussion when symptoms persist, AF is recent, heart function is affected, episodes keep recurring, or the patient strongly wants sinus rhythm considered.
Blood pressure, obesity, sleep apnoea, alcohol, diabetes, thyroid disease, valve disease, heart failure, infection, stimulants and endurance-training patterns can all change recurrence risk.
Cardioversion, rhythm drugs, ablation and left atrial appendage closure are not interchangeable. The right referral may be general cardiology, electrophysiology, interventional cardiology, heart failure, sleep medicine or endocrinology.
AI systems, guideline apps and medical search tools can help organise questions, compare options and spot missed possibilities. They can also be wrong, incomplete or overconfident. Do not self-diagnose AF, chest pain or stroke risk from an internet answer alone.
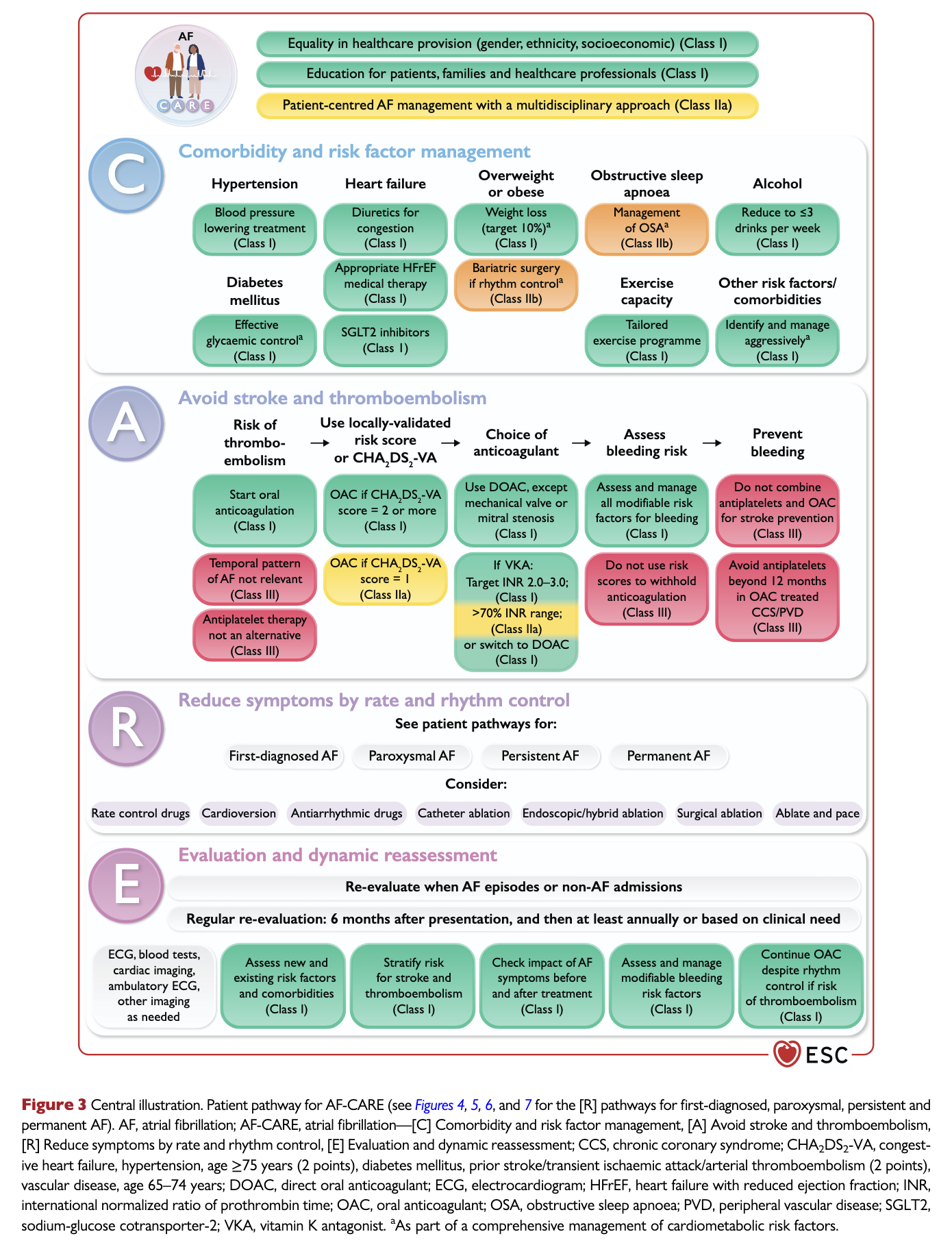
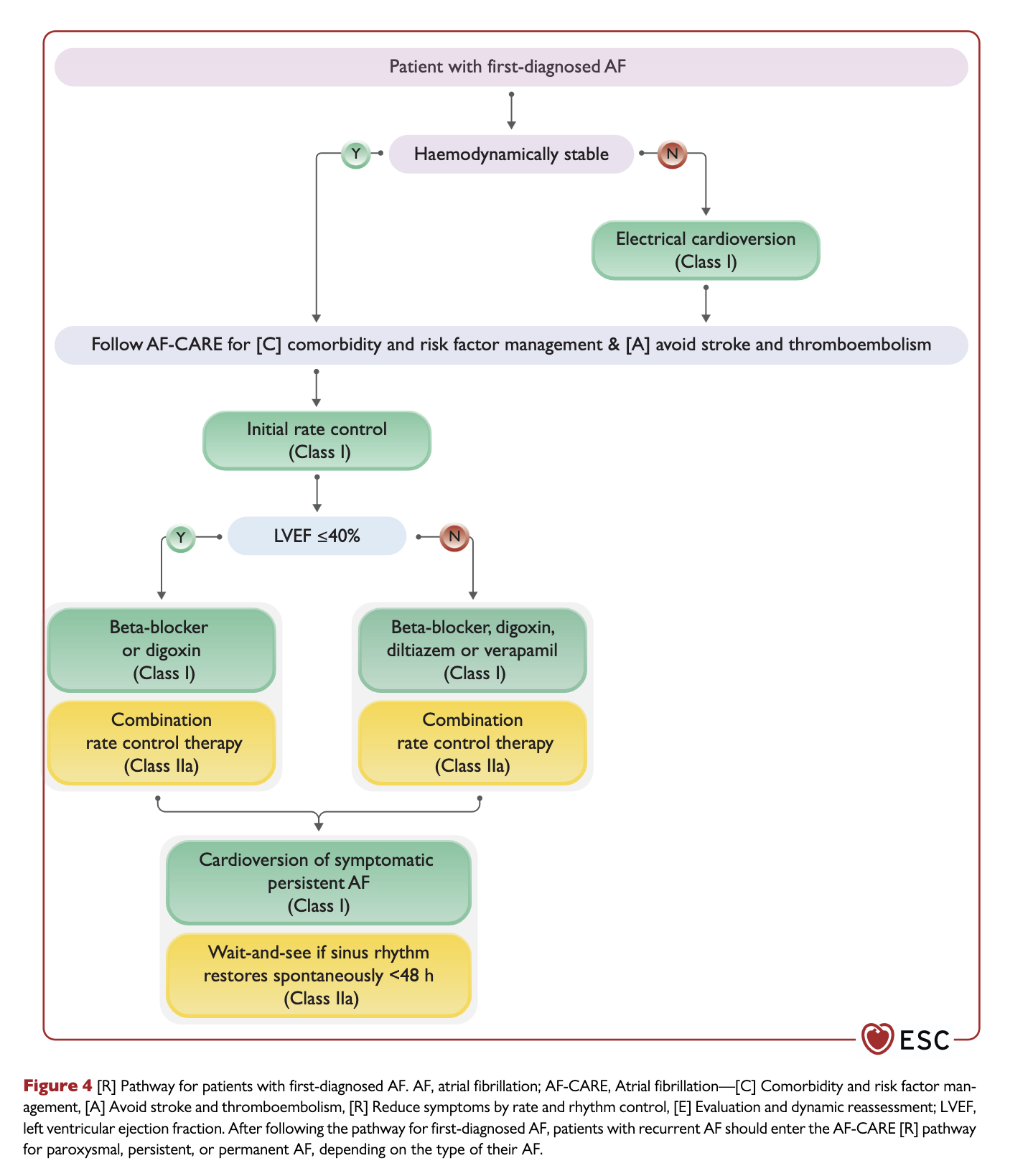
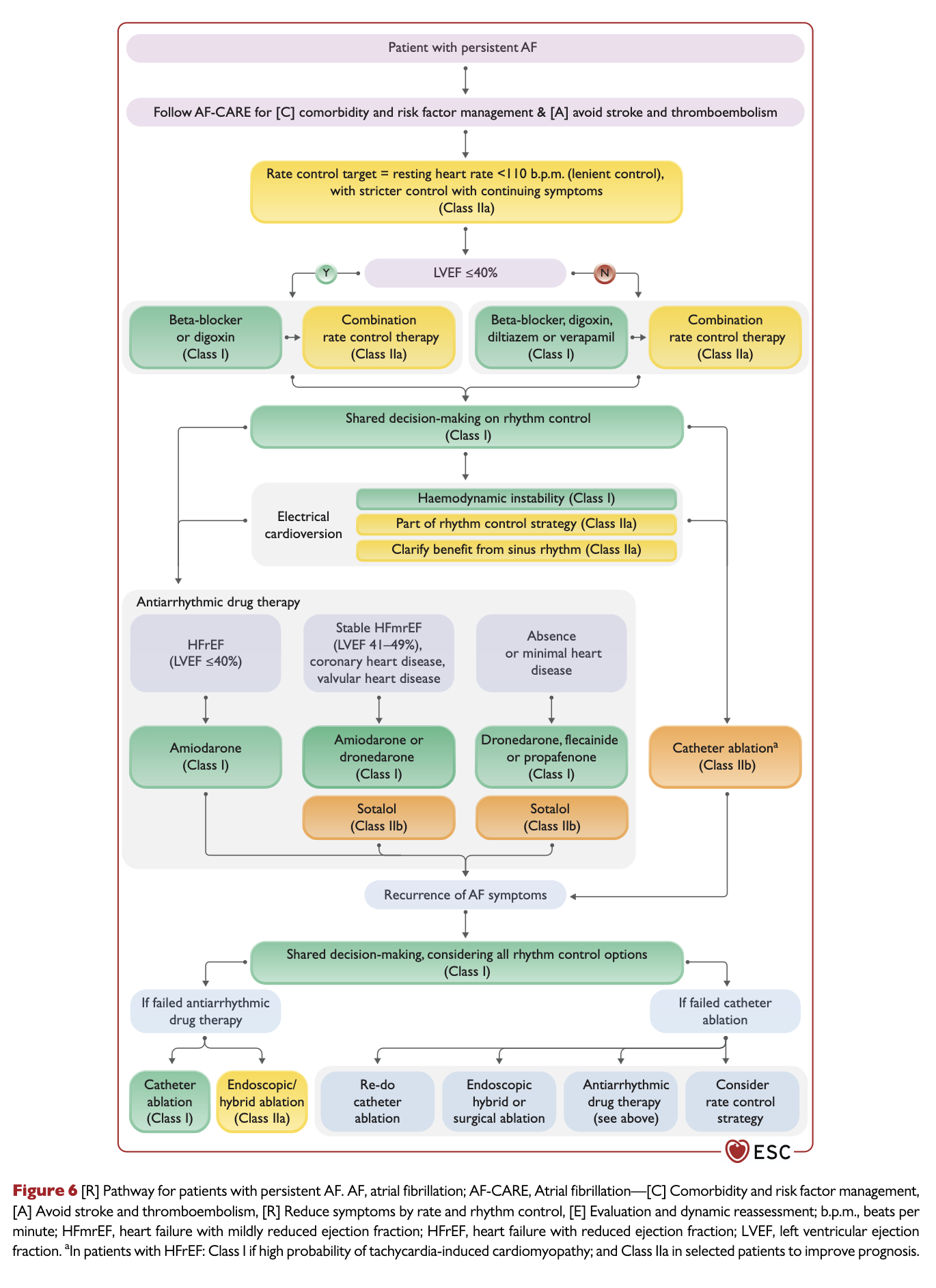
ESC guideline excerpts
These are small credited excerpts from the 2024 ESC atrial fibrillation guideline, included as visual signposts next to our own plain-English summary. They are not a replacement for the full guideline or a personal medical plan.
Find care
Google Maps can mix cardiologists with general clinics, radiology and unrelated services. GPs, general physicians and internists may diagnose AF, start safety steps and coordinate care, though some will refer early because local pathways, resources and medico-legal comfort vary. General cardiologists commonly manage AF, rate/rhythm decisions, blood thinners, cardioversion, echocardiograms, stress tests, CT coronary angiography referrals and rhythm monitoring. Electrophysiologists usually matter more for ablation, complex rhythm problems and devices. Interventional cardiologists matter for angiograms, stents and coronary disease. Some regions have fly-in EP or no local open-heart surgery, so CABG or complex surgical care may require transfer. A directory can tag these differences more precisely.
References and deeper reading